Obstacles and disparities associated with health equity impact all elements of health, including cancer screening. For colorectal cancer (CRC) screening, nearly half of premature CRC deaths nationwide are related to racial/ethnic, socioeconomic, and geographic inequalities.1 Data on health inequities and disparities is a key tool for identifying and addressing these barriers in vulnerable populations, thus improving health equity.
33%
Increased chance of black/African American individuals dying from colorectal cancer than White individuals2
20%
Amount of deaths caused by all cancers in Hispanic individuals – the leading cause of death for this group3
23%
Higher risk of colorectal cancer mortality for those living in rural areas compared to people with colorectal cancer living in urban areas4
|
Black and African American2 |
Hispanic and Latino3 |
American Indian/Alaska Native |
|
|
|
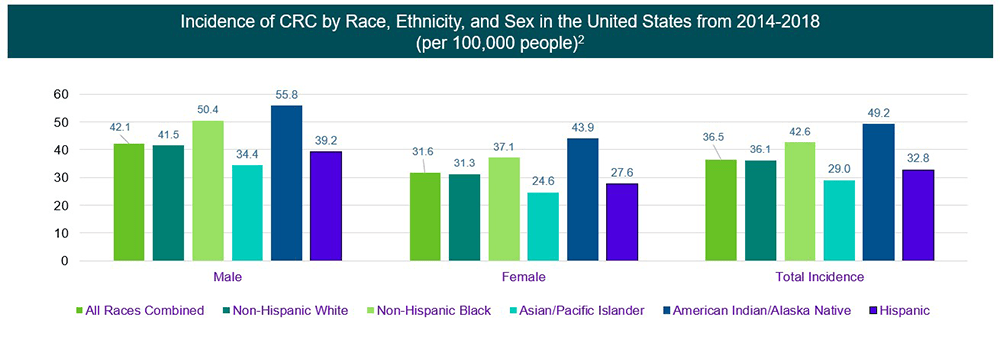
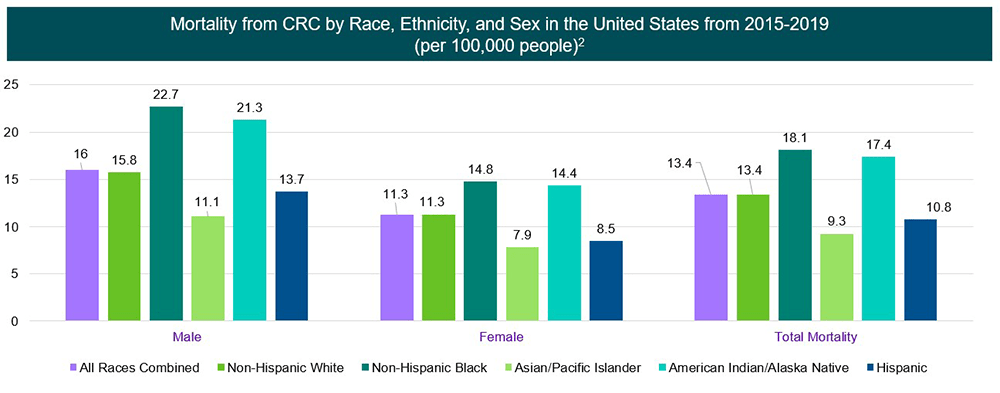
- CRC incidence was highest among American Indian/Alaskan Natives, while CRC mortality was highest among Non-Hispanic Blacks
- Incidence and mortality vary widely across populations
- These differences vary by sociodemographic characteristics, which are influenced and perpetuated by social determinants of health
- Race categories represented capture a large heterogeneity of individuals and origins [US Census]
Last Updated: 4/25/2023
References
1 Jemal A, Siegel RL, Ma J, et al. Inequalities in premature death from colorectal cancer by state. J Clin Oncol. 2015;33(8):829-835
2 Siegel RL, Miller KD, Waggle NS. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48
3 ACS. Cancer facts & figures for Hispanic/Latino People 2021-2023. Atlanta: American Cancer Society. 2021
4 CDC. An Update on Cancer Deaths in the United States. [updated February 28, 2022, Accessed April 25, 2023. https://www.cdc.gov/cancer/dcpc/research/update-on-cancer-deaths/index.htm
5 Melkonian SC, Weir HK, Jim MA, et al. Incidence of and trends in the leading cancers with elevated incidence among American Indian and Alaska Native populations, 2012-2016. Am J Epidemiol. 2021;190(4):528-538
Footnotes
aBased on people with CRC in stage I, stage IIa, or stage IIb between 2012 and 2018.
bPer American Joint Committee on Cancer’s (AJCC) staging system: Localized = stage I, IIa, IIb. Regional = stage IIc and III. Distant = stage IV.3