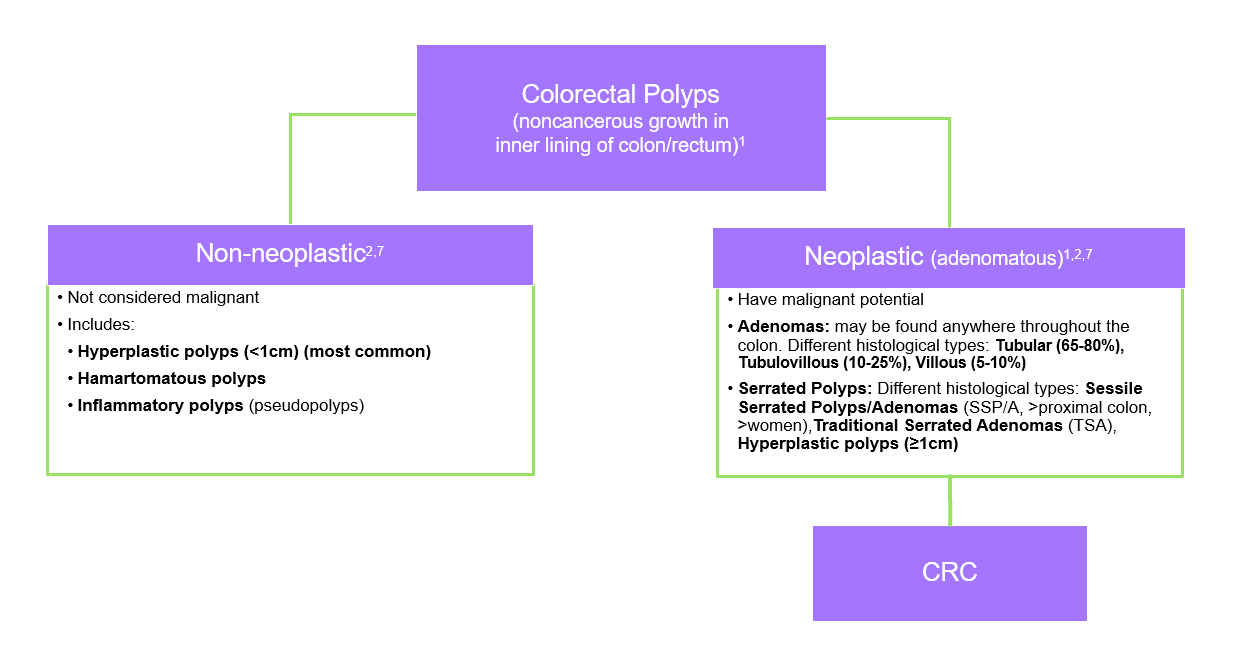
Colorectal lesions may be cancerous or noncancerous polyps. Some polyps that begin noncancerous may still hold malignant potential and become cancerous (adenomas and serrated polyps).1,2
~70% OF CRC DEVELOPS FROM ADENOMAS3
The evolution of colorectal adenoma to early-stage CRC typically takes more than 10 years, providing an important opportunity for screening and early detection3,4
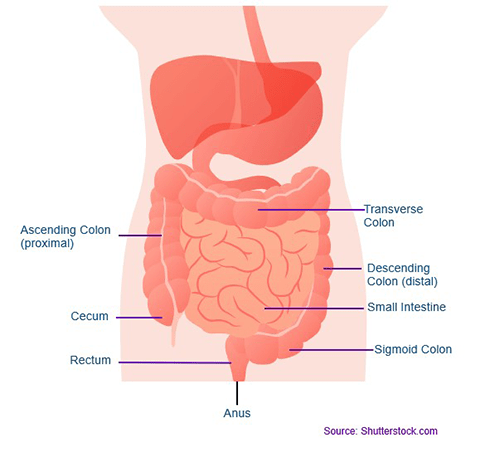
Basic Anatomy of Colon and Rectum
Source: Shutterstock.com
• The colon begins at the cecum and is divided into 4 parts:1
- Ascending
- Transverse
- Descending
- Sigmoid
Understanding Colon Pathology
Stages Of Colorectal Cancer
- CRC usually begins as a polyp1
- When a polyp progresses to cancer, it can grow into the wall of the colon/rectum (local)1
- It may invade lymph vessels and spread to nearby lymph nodes (regional)1
- Cancer cells may also be carried via blood vessels to other organs such as the liver or lung (distant)1
- Exfoliation of cellular material occurs in advanced adenoma and CRC that is not seen in normal mucosa5
Right-Sided Vs. Left-Sided CRC6,8
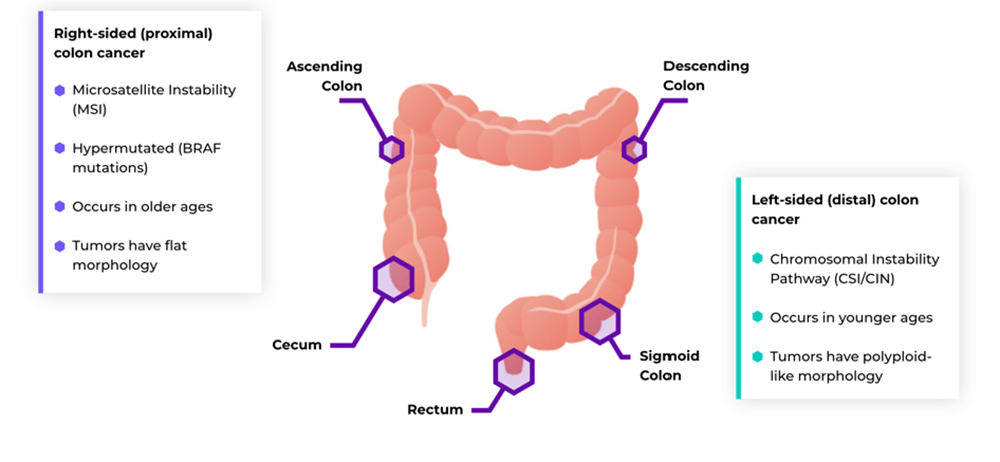
Characteristic features of CRC by anatomic subsite6 |
|
|---|---|
| RIGHT-SIDED (PROXIMAL) CRC | LEFT-SIDED (DISTAL) CRC |
| Mucinous adenocarcinomas, sessile serrated adenomas | Tubular, villous adenocarcinomas |
| Flat like morphology | Polypoid like morphology |
| MSI-high and mismatch repair deficient tumors | CIN-high tumors |
| Highly immunogenic, high T cell infiltration | Low immunogenic |
| Metastases in peritoneal region | Liver and lung metastases |
| More common in >50 y.o. | More common in <50 y.o. |
| Predominantly occur in females | Predominantly occurs in males |
| Better prognosis at early stages (stage I and II) | Better prognosis at late stages (stage III and IV) |
References
1 American Cancer Society. Colorectal cancer facts & figures 2023-2025. Atlanta: American Cancer Society; 2023.
2 Shussman N, Wexner SD. Colorectal polyps and polyposis syndromes. Gastroenterol Rep. 2014;2(1):1-15.
3 Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2017;112(7):1016-1030.
4 Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterol. 1997;112:594-642.
5 Geenen DJ, et al. A 3-year observational study of persons with a negative colonoscopy and positive multi-target stool DNA test, 2017. Poster presented at: Digestive Disease Week (DDW); 6-9 May 2017; Chicago, IL.
6 Baran B, Mert Ozupek N, Yerli Tetik N, et al. Difference between left-sided and right-sided colorectal cancer: a focused review of literature. Gastroenterol Res. 2018;11(4):264-273.
7Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update buy the US Multi-Society Task Force on colorectal cancer. Gastrointest Endosc. 2020;91(3):463-485.e58 Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48.
Last Updated: 5/30/2023